
Is AI a Tool or a System? Why the Answer Reshapes Every Decision Health Plans Make
The dominant model of AI adoption in health plans, point solutions procured tool by tool, produces diminishing returns. The organizations that pull ahead will treat AI as core infrastructure, not instrumentation.
Introduction
Across health plans and health systems, the same question is surfacing in boardrooms and technology committees: Are we deploying AI, or are we building an AI-enabled organization? The distinction sounds semantic. It is anything but.
Currently, artificial intelligence enters healthcare through a succession of point solutions; a predictive model here, a risk stratification tool there, supplemented by an agentic AI pilot. Each promises measurable value in isolation. Some deliver a little value, but most underwhelm. The cumulative effect is a landscape of disconnected capabilities that do not compound, do not learn from one another, and do not fundamentally change what a health plan can do.
The organizations that will pull ahead are not the ones with the most AI tools. They are the ones that will start building AI as core infrastructure. They have stopped thinking in silos and started designing automation that flows end to end with a focus on how AI gets deployed to drive outcomes that truly move the needle across the entire plan.
In this article, we will illustrate that the tool-versus-system distinction is the most consequential strategic choice facing health plan leadership today - and that most organizations do not yet realize they can't delay.
Overview
- The dominant model of AI adoption in health plans (point solutions procured tool by tool) produces diminishing returns and structural fragility. It optimizes individual pilots without transforming organizational capability.
- A systems approach to AI treats prediction, outreach, intervention, and outcome measurement as a closed loop. Each element informs the others. The organization learns continuously rather than in discrete procurement cycles.
- The distinction has immediate and compounding implications for workforce design, vendor strategy, data governance, and the relationship with providers.
- Health plans that make this transition intentionally will define what a health plan looks like in the next decade. Those that do not will find themselves at a perpetual disadvantage.
- The barriers to transition are part technical but much more importantly they are organizational. They require a clear executive decision about what kind of AI organization your health plan intends to become, and the discipline not to defer that decision indefinitely.
The Tool Paradigm and Its Limits
The tool paradigm has a coherent logic. A health plan identifies a high-cost problem, for example, avoidable emergency department utilization among members with complex chronic conditions. It procures a predictive model designed to identify that population. The model surfaces a list. Case managers work the list. Results are measured. The tool either gets renewed or replaced.
This approach is not wrong. It is simply insufficient for the competitive and regulatory environment health plans now face. The fundamental problem is that AI tools, procured and operated in isolation, cannot compound. A risk stratification model that does not talk to an engagement platform cannot learn which high-risk members are actually reachable. An engagement platform that does not feed back into the predictive model cannot improve its own targeting. A care management workflow that does not connect to outcomes data cannot know whether the interventions it prioritized were the right ones.
The result is a form of organizational amnesia. Each engagement cycle begins roughly where the last one ended. This is not because the data does not exist, but because the architecture was not built to learn from it. As a result, these investments never flow to pricing or network or anything else that enables the health plan to operate on a differentiated plane. A study from MIT's NANDA initiative found that 95% of enterprise AI pilots fail to deliver measurable ROI - not because algorithms are flawed, but because they are poorly integrated and misaligned with real-world workflows.
There is also a workforce dimension that rarely surfaces in vendor conversations. When clinical and operational staff operate within a tool paradigm, they become skilled at working individual tools, interpreting a risk score, navigating an engagement platform, documenting in a care management system. They do not develop the institutional knowledge that comes from operating inside a system where those tools speak to one another. The human expertise and technological capability develop in parallel rather than in combination.
The result, as one health plan CMO described it, is "AI that makes us more efficient at the wrong things."
What a System Actually Looks Like
A systems approach does not focus on solving each problem in isolation. It asks how automation integrates across the organization to produce a fundamentally different operating model, one that gets smarter with every cycle. In a well-designed AI system, predictive identification is not a starting point, it is one part of a continuous cycle. Take a simple example and one that health plans do all the time, often with little tangible ROI: outreach to high-risk members. In a tool paradigm, this is a list-management exercise. In a system, it becomes a closed loop.
A member is identified as high-risk. The system determines the optimal outreach channel and timing based on prior engagement data for that member and comparable members. An AI-enabled outreach agent contacts the member. The response (or non-response) updates the member's engagement profile. The care manager who follows up has access not just to a risk score but to a record of what has already been tried, what worked, and what the member's actual preferences appear to be. The intervention that results is documented in a way that feeds back into the predictive model. The model improves.
But the loop does not close at the care manager. That same information flows to three additional destinations that most tool-paradigm deployments never reach: to product and clinical teams to inform plan design; to the actuarial team to sharpen pricing assumptions; and back to provider EMRs to close the clinical loop. Automation that stops at care management is automation that has captured a fraction of its available value.
This is not a description of technology. It is a description of organizational design. The loop only closes if the architecture, the data governance, the workflow design, and the human roles are all structured around closing it. Any break in the chain and the automation was a nice pilot, but it won't impact a health plan's administrative costs, the cost of care or the quality/experience the member has.
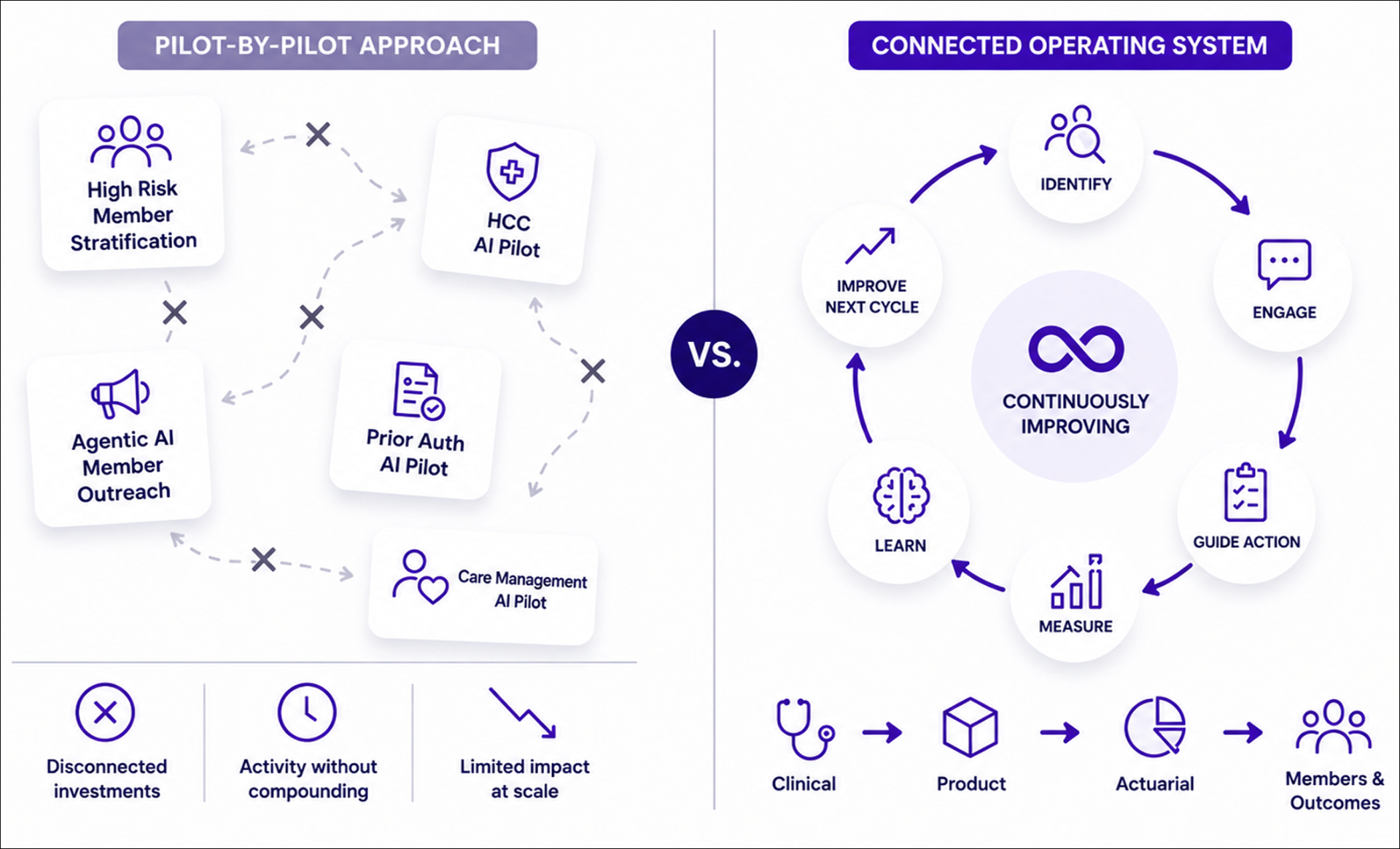
Our experience across payer deployments has reinforced a simple lesson: the value of AI rarely comes from any one capability in isolation. A strong prediction model can still fail if the plan cannot reach the member. An outreach agent can still underperform if it is not connected to the right workflow. A workflow tool can still create limited value if outcomes are not measured and fed back into the next decision. The deployments that work best are the ones designed as a closed loop from the beginning: identify the opportunity, engage the right person, guide the next action, measure what happened, and use that learning to improve the next cycle. That is where AI starts to become infrastructure rather than instrumentation.
Sharp HealthCare's Chief Digital Officer recently said - and it applies equally to health plans: "We'll move from point solutions that solve individual problems to platforms that support many use cases." The era of one-off AI tools is ending; 2026 is defined by consolidation into integrated ecosystems.
The implications for vendor strategy are significant. Health plans operating in the tool paradigm tend to procure point solutions and attempt integration after the fact. A process that rarely works well. Health plans building toward a system architecture tend to focus on a much more holistic approach to automation, but equally as important, to the integration and deployment. Some have called in Big Tech to help but again this is a strategy that rarely works because they don't understand the nuances of healthcare and how to build the operational workflows necessary for a successful deployment. This approach is overwhelming to many leaders so they say things like "let's take baby steps first" or "let's pilot". A pilot is an expensive way of delaying a decision. Some leaders worry that they won't see immediate results but those that apply a system approach find that the long-term advantage is decisive.
The Strategic Implications for Health Plan Leadership
The tool-versus-system distinction is not primarily a technology question. It is a governance question, a workforce question, and a contracting question. Each domain is affected in ways that compound over time.
Governance
Tool-paradigm organizations tend to govern AI at the departmental level. Medical management buys its tools, IT buys its infrastructure, and analytics buys its models. A systems approach requires cross-functional governance with executive authority. Someone at the health plan must own the loop, not just the individual nodes. Ideally the responsible executive needs to be the CEO's right hand - whether that be the President, COO or CFO. However, where it sits matters much less than whether it exists at all.
Workforce
The health plan workforce is the most visible casualty of the tool paradigm and the most significant beneficiary of the system transition. In a tool environment, they are task executors. They work lists, and escalate exceptions. In a system environment, the workflow is proactively designed to integrate care management with UM with claims operations and contact centers. Risk adjustment and provider operations benefit from the same information that flows to Quality outreach and enrollment. All this feeds back to product design, network and pricing. The deployment of AI for a health plan is not a point solution designed for headcount reduction. It is an entire role redesign. Health plans that execute on this strategy will have a significant competitive advantage.
Value-Based Contracting
One of the implications of the tool-versus-system distinction is its effect on a health plan's ability to take and perform on value-based risk. Point solutions can improve the efficiency of operations at the margin. System-level AI can change the expected value of a risk contract. A health plan that can predict with confidence which members will drive cost, engage them reliably, and intervene effectively is operating with a fundamentally different actuarial profile than one that cannot. As value-based care penetration continues to accelerate, with CMS projecting that the majority of Medicare beneficiaries will be in some form of accountable care arrangement by 2030, the health plans with system-level AI capability will be structurally positioned to absorb risk their competitors cannot.
The Transition: Less Technical Than It Appears
Health plan leaders who recognize the tool-versus-system distinction often assume the barrier to transition is technical. They believe that moving from a collection of AI tools to a functioning AI system requires infrastructure investments that are years away. They have a misguided belief that they need to spend years pulling data from a mainframe and organize it in a data lake and then think about automation. Health plans do not need another data swamp. In practice, the more common barrier is organizational clarity.
The technical components of an AI system exist today. It is whether a health plan's leadership has made a clear decision to assemble them in a way that will drive a moment in time or a transformation.
That decision involves trade-offs that are genuinely difficult. It requires health plan leadership to resist the procurement logic that produces tool sprawl. Every health plan leader has experienced the pressure to adopt whatever point solution promises the best outcome on the metric that is currently under scrutiny. It requires investment in data governance that does not produce short-term ROI. It requires a vendor strategy that values integration and deployment. And it requires an honest organizational assessment: what is the plan's current AI capability, what is the intended destination, and what is the transition path?
None of this is beyond the capacity of a well-led health plan. But it requires the kind of intentional executive decision-making that the tool paradigm, paradoxically, tends to defer. When each AI purchase is justified on its own merits, the question of what kind of AI organization the health plan intends to become never quite reaches the agenda. The longer a health plan continues on this misguided path, ironically the harder it is to implement a system strategy.
What Should We Do on Monday Morning?
Figuring out how or where to start can be daunting. However, like running a marathon, if you don't start running the early miles you will never finish. The plans that are building system-level AI today are not the ones that had a perfectly sequenced data strategy three years ago. They are the ones that picked a high-value use case, designed the closed loop around it, deployed it, measured it, and moved to the next one.
The most common mistake at this stage is starting with data. There is a substantial graveyard of data consolidation projects that consumed years of effort and produced limited operational value. Data work that is not in service of a defined use case tends to produce reports, not decisions.
A more productive starting point: identify the top five highest-cost, highest-variability problems in the plan. Select one. Design the full automation loop around it: prediction, engagement, intervention, outcome measurement, and feedback. Deploy it. Use what you learn to improve the loop while standing up the next one. This approach builds organizational capability incrementally and visibly, creates a cycle of internal proof points, and generates the institutional knowledge that makes each subsequent deployment faster and more effective.
The goal of the first use case is not ROI in isolation. It is demonstrating that the organization can design, deploy, and learn from a closed loop. The capacity to build and improve AI systems rather than simply procure AI tools is the durable competitive asset.
Conclusion
The history of transformative technology in complex industries follows a consistent pattern. Early adoption is characterized by the deployment of individual tools that improve existing workflows. The organizations that ultimately define the competitive landscape are those that recognize, early enough, that the technology can restructure the workflow itself and make the organizational investments required to capture that capability.
Healthcare AI is at that inflection point. The question of whether AI is a tool or a system is not an abstract strategic framing. It is the question that will determine which health plans are setting the standard in 2030 and which are struggling, trying to play catch up at a continuous structural disadvantage.
The answer does not require a technology breakthrough. It requires a decision. Throughout history, new technology has led to new business models. At the beginning of the internet how many people envisioned the need for logistics companies, last mile delivery businesses or cloud computing. Similarly, automation in healthcare won't just bring headcount efficiencies, it will drive fundamentally new business models. Health plans can take the lead and transform themselves or sit back and watch it happen to them.
McKinsey framed the stakes plainly: "Payer CEOs should consider if they want to lead or follow. The size of the opportunity suggests that those who choose to wait will need to have a ready response plan if competitors move ahead successfully. For example, followers could find themselves in a position where industry leaders have 10 percent lower medical costs or 20 percent lower administrative costs, a daunting prospect."
This gap compounds with every cycle in which one organization learns and another does not. This decision requires leadership. It will define the future of your organization.
Endnotes
- MedCity News, "Healthcare's AI Illusion: Why Integration, Not Algorithms, Will Define the Next Decade," January 2026.
- Interview with health plan Chief Operating Officer, conducted under Chatham House rules, Q2 2026.
- Becker's Hospital Review, "How the AI Conversation Will Change in 2026," December 2025.
- Centers for Medicare & Medicaid Services, "CMS Innovation Center Strategy Refresh," 2024. CMS projections indicate continued growth in accountable care participation, with stated goals for majority Medicare beneficiary enrollment in alternative payment models.
- Diagnostic Robotics internal analysis, 2026. Based on structured assessment of health plan AI readiness across predictive capability, engagement infrastructure, data governance, and workflow integration dimensions.
- McKinsey & Company, "The AI opportunity: How payers can capture it now," 2024. The report documents that payers who make the right digital and AI investments will have an advantage worth hundreds of millions of dollars.
All Rights Reserved. This brief does not constitute clinical, legal, or investment advice. The unauthorized reproduction or distribution of this material is prohibited.